
The critical shortage of maternal healthcare services in rural Alabama has reached a tipping point, forcing state officials to implement a radical technological solution to prevent rising mortality rates among expectant mothers. This crisis is particularly acute in the state’s expansive rural regions, where the disappearance of labor and delivery wards has left thousands of women without local access to life-saving prenatal care. To bridge this geographic and medical chasm, the Alabama Rural Health Transformation Program was established as an ambitious multi-million-dollar initiative. By integrating cutting-edge robotic ultrasound systems into local clinics, the program seeks to provide high-level diagnostic capabilities to areas that have long been neglected by the traditional healthcare system. This strategy represents a significant shift in how public health is managed, placing the state at the forefront of a high-stakes experiment that tests whether sophisticated machinery can compensate for a lack of human specialists in isolated communities.
Remote Diagnostics: The Mechanics of Tele-Robotic Care
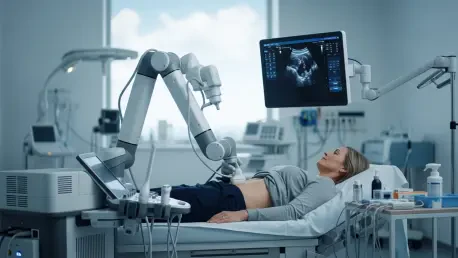
The operational core of the state’s new health initiative centers on the deployment of tele-robotic ultrasound machines to various rural counties that currently lack resident obstetricians or maternal-fetal medicine specialists. These advanced systems allow medical experts located at urban academic centers, specifically the University of Alabama at Birmingham, to perform detailed prenatal scans from a significant distance. Using a specialized interface, the remote physician can control the movement of the ultrasound transducer on the patient’s abdomen in real-time, receiving high-definition imagery that is critical for assessing fetal development. This technological bridge is designed to bring the expertise of a Tier-1 medical facility into the heart of the “Black Belt” and other underserved regions. The primary objective is to replicate the precision of an in-person specialist visit without requiring the patient to undertake a grueling multi-hour journey to a major city for a routine screening.
Beyond the basic imaging capabilities, these robotic systems are equipped with sophisticated sensors that provide haptic feedback to the remote operator, ensuring that the pressure and angle of the scan are both safe and effective. This level of technical sophistication is necessary to identify complex conditions such as placenta previa, fetal growth restriction, or congenital heart defects that might otherwise go unnoticed in a standard clinic setting. By catching these high-risk complications during the early stages of pregnancy, the program aims to proactively manage patient care and coordinate necessary interventions before a medical emergency occurs. This approach emphasizes the preventive potential of telemedicine, moving beyond simple video consultations to a more tactile and diagnostic form of remote interaction. The goal is to establish a standard of care in rural Alabama that matches the diagnostic rigor found in urban hospitals, effectively neutralizing the disadvantage of geographical isolation for expectant mothers.
The Geographic Crisis: Survival in the Obstetric Desert
The necessity of this technological intervention is underscored by the sobering reality of Alabama’s healthcare infrastructure, where fifty-eight of the state’s sixty-seven counties are classified as rural. Within this landscape, thirty-six counties currently operate without any specialized obstetrics care, and forty-one counties lack a single facility capable of providing labor and delivery services. This vast “obstetric desert” has created a situation where pregnant women must travel an average of forty-five minutes to over an hour just to reach a hospital equipped for childbirth. Such long travel times are not merely an inconvenience; they are a direct threat to maternal and infant safety, particularly when complications arise unexpectedly. The systemic withdrawal of medical services from rural areas has left a vacuum that traditional recruitment efforts have failed to fill, prompting state leaders to look toward federal funding and innovative engineering as the only viable path forward for the state’s residents.
Current health outcomes in Alabama reflect the severity of this lack of access, with the state recording some of the highest maternal mortality rates in the nation. Recent data indicates nearly sixty deaths per one hundred thousand live births, a statistic that state officials describe as an untenable failure of the existing system. Governor Kay Ivey and other proponents of the transformation program argue that the status quo cannot be maintained, and that the modern health infrastructure must adapt to the physical realities of the region. By utilizing federal resources made available through recent legislative acts, the state is attempting to modernize its rural clinics to prevent the further escalation of this mortality crisis. The initiative is not just about installing machines; it is about responding to a historical decline in rural medical investment that has disproportionately affected low-income and minority populations. Without these interventions, the gap between urban and rural health outcomes would likely continue to widen.
Connectivity Barriers: Addressing the Digital Divide
While the promise of robotic medicine is substantial, the successful implementation of the program faces significant hurdles related to the state’s existing physical and digital infrastructure. High-definition robotic ultrasounds require exceptionally stable and high-speed internet connections to transmit complex medical data and video feeds in real-time without latency. In many of Alabama’s most impoverished rural counties, broadband access remains inconsistent or entirely unavailable, posing a risk that the technology may fail at critical moments. Experts in rural health research have pointed out that a “digital divide” could inadvertently leave the most vulnerable patients behind if the underlying telecommunications network is not fortified alongside the medical equipment. For the robotic initiative to be effective, it must be supported by a robust ecosystem of high-speed connectivity that can handle the massive bandwidth requirements of modern diagnostic tools across the state.
In addition to technological requirements, the human element of the program remains a critical bottleneck that machinery alone cannot resolve. Even with a robot performing the scan, a trained healthcare worker must be physically present at the rural clinic to assist the patient, manage the equipment, and provide immediate emotional or physical support. Alabama continues to face a chronic shortage of nurses and technicians in rural areas, meaning that finding the staff to operate these satellite clinics is just as difficult as recruiting doctors. Critics of a purely technological approach argue that the focus should remain on human capital, as a robot cannot replace the holistic care provided by a midwife or a nurse practitioner. The success of the Alabama Rural Health Transformation Program will therefore depend on a balanced strategy that pairs sophisticated robotics with intensive training programs for local healthcare workers, ensuring that the technology is an enhancement of care rather than a lonely substitute for it.
Systemic Limitations: Moving from Diagnosis to Intervention
A fundamental challenge raised by local medical practitioners is the distinction between providing a diagnosis and delivering actual medical treatment. While a robotic ultrasound might successfully identify a life-threatening complication in a rural patient, the discovery of the problem does not automatically solve the issue of geographical distance from a surgical suite. If a woman is diagnosed with a condition requiring an emergency cesarean section or immediate hospitalization, she still faces the original problem of being miles away from a functioning labor and delivery ward. Identifying a high-risk pregnancy via a remote robot is a vital first step, but without local facilities to provide the necessary follow-up care, the technology may simply serve to highlight the systemic gaps in the state’s medical network. The “last mile” problem remains a significant concern for those who believe that technology must be backed by a restoration of physical hospital services in the rural South.
The program has also become a focal point for a larger national debate regarding the direction of American healthcare policy and the role of innovation. Proponents of the initiative, including federal health administrators, view the use of robotics as a brilliant application of American medical excellence to reach populations that have been “left behind” by traditional models. They argue that if doctors cannot be convinced to move to rural areas, the expertise must be sent there electronically. Conversely, some national leaders view the reliance on robots as a symptom of a failed system that prioritizes high-tech fixes over fundamental investments in doctors, midwives, and community clinics. This tension between technological optimism and the demand for human-centered medical investment defines the current landscape of the Alabama experiment. Whether the robotic initiative is seen as a revolutionary success or an expensive stopgap will ultimately depend on its ability to integrate with a broader, more comprehensive strategy for rural health.
Future Pathways: Establishing Sustainable Rural Networks
The initial phase of the Alabama Rural Health Transformation Program established a critical framework for addressing maternal health disparities through integrated technology. State officials moved beyond the pilot stage by authorizing the distribution of emergency labor and delivery carts to rural hospitals, ensuring that even facilities without dedicated obstetric wings possessed the tools to stabilize patients in crisis. This broader focus indicated that the state recognized the limitations of robotics when used in isolation, opting instead for a layered approach that combined remote diagnostics with physical emergency readiness. Practitioners participated in comprehensive training modules that allowed them to coordinate more effectively with urban specialists, creating a streamlined referral network that prioritized high-risk cases for immediate transport. This systemic coordination provided a necessary safety net for women who previously lacked any connection to the specialized care found in metropolitan medical hubs.
Strategic improvements in regional broadband infrastructure were prioritized to ensure that the tele-robotic systems functioned without interruption in the state’s most isolated counties. Local governments collaborated with telecommunications providers to create high-priority data corridors for medical facilities, successfully reducing the latency issues that had previously hindered remote imaging. Furthermore, the state introduced new scholarship and incentive programs aimed at recruiting ultrasound technicians and nurse practitioners to staff these specialized rural hubs, addressing the human capital shortage that threatened the program’s long-term viability. By focusing on both the digital and physical components of care, Alabama provided a blueprint for other states facing similar rural healthcare collapses. Future initiatives will likely focus on expanding these remote capabilities to include other specialties, such as cardiology and neurology, ultimately transforming the rural clinic from a limited outpost into a sophisticated portal for world-class medical expertise.







