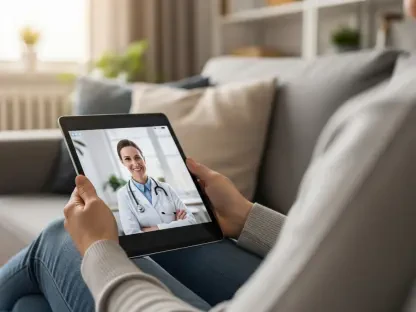

Recent data analyzed by researchers at King’s College London indicates that approximately 14% of the adult population in the United Kingdom has transitioned from traditional medical consultations to utilizing artificial intelligence chatbots for primary health concerns. This shift is not merely a technological curiosity but a direct response to the mounting systemic pressures facing the National Health Service (NHS), where extensive waiting lists and administrative delays have become commonplace. For many, the immediacy of a digital interface outweighs the frustration of waiting weeks for a general practitioner appointment, providing a sense of agency in a strained system. While over half of those who have integrated AI into their health management report positive outcomes regarding their physical and mental wellbeing, the trend raises profound questions about the future of clinical governance and the boundaries of automated medical advice. The convenience of 24/7 accessibility has turned smartphones into the first line of defense for a significant portion of the public, altering the fundamental patient-doctor relationship.
Demographic Disparities: Skepticism Among Younger Populations
A counterintuitive finding in recent behavioral studies is the notable demographic divide regarding the acceptance of clinical AI, particularly among those traditionally viewed as tech-savvy. Women and individuals aged 18 to 24 represent the most skeptical cohorts, often expressing higher levels of opposition to the integration of automated systems within the NHS compared to older generations. This group challenges the prevailing assumption that technological familiarity naturally equates to trust, suggesting that younger users are more acutely aware of the nuances lost when human interaction is removed from healthcare. Their hesitation often stems from concerns regarding data privacy, the lack of personalized empathy, and the potential for algorithmic bias to affect marginalized groups. This resistance highlights a critical gap between the rapid deployment of health technology and the public’s readiness to entrust their long-term medical safety to non-human entities, necessitating a more transparent approach to how these systems are developed and vetted for public use.
The divergence in opinion between age groups suggests that older adults might perceive AI as a necessary utility to bypass logistical hurdles, whereas younger demographics view it through a lens of digital ethics and quality of care. Such a split indicates that a one-size-fits-all implementation strategy for AI in the healthcare sector is likely to face significant friction. Building trust among younger skeptics requires more than just functional improvements; it demands rigorous evidence of clinical accuracy and clear ethical frameworks. As long as these populations feel that AI is being used as a cost-cutting measure rather than a tool for genuine clinical enhancement, the adoption rate among those who will inherit this system may remain stagnant. Addressing these concerns is vital because the long-term sustainability of digital health initiatives depends on the buy-in of the next generation of patients and healthcare providers. Consequently, developers must prioritize user-centric design that acknowledges these specific social and ethical anxieties rather than dismissing them as mere technophobia.
Safety Implications: The Risks of Bypassing Professional Triage
The reliance on generative models for health inquiries introduces substantial safety risks that extend beyond simple misinformation, as approximately 21% of users have avoided seeking professional medical help based on chatbot feedback. Clinical studies published in journals like Nature Medicine emphasize that while these bots are adept at synthesizing general information, they frequently fail to accurately triage life-threatening emergencies or identify complex mental health crises. For instance, a chatbot might suggest home remedies for symptoms that a trained physician would recognize as early indicators of cardiac distress or severe neurological issues. This gap in diagnostic capability is particularly dangerous because the authoritative tone of AI responses can instill a false sense of security in the user. When a patient opts for a digital interaction over a physical exam, the subtle physical cues—such as skin turgor, pupil response, or localized tenderness—that are essential for an accurate diagnosis are completely omitted from the clinical picture.
Furthermore, the current generation of AI tools is not universally equipped to handle the intricacies of suicidal ideation or profound psychological trauma, where human empathy is not just a comfort but a clinical necessity. Experts from the Medicines and Healthcare products Regulatory Agency (MHRA) have pointed out that while AI can streamline information access, it lacks the nuanced judgment required to navigate the gray areas of medicine. The risk of “silent misdiagnosis” grows as more individuals treat these platforms as definitive diagnostic tools rather than supplementary information sources. Without the intervention of professional expertise, minor conditions can escalate into chronic issues, and acute emergencies may be missed entirely. The push toward digital health must therefore be balanced with clear guardrails that prevent these tools from being used as a complete substitute for human oversight. Protecting public health in this new landscape requires a collaborative effort between technologists and clinicians to ensure that AI serves as a bridge to professional care rather than a barrier that keeps patients away from the clinic.
Future Outlook: Enhancing Digital Literacy and Regulatory Oversight
Moving forward, the focus must shift toward comprehensive public digital literacy campaigns that educate users on the specific limitations of large language models in a medical context. Rather than attempting to halt the adoption of AI, regulatory bodies should implement standardized labeling and “health-safe” certifications for chatbots to help the public distinguish between verified medical aids and general-purpose conversational tools. It is essential for users to understand that an AI’s primary function is pattern recognition, not clinical reasoning; therefore, it should be utilized strictly for preliminary research or administrative assistance, such as scheduling or general wellness tracking. Strengthening the partnership between the NHS and technology developers will be crucial in creating integrated systems where AI acts as a smart triage layer that fast-tracks urgent cases to human doctors rather than replacing them. This strategy would address the core issue of waiting times while maintaining the high standard of care that only professional medical staff can provide.
The evolution of healthcare in this decade was characterized by a rapid, often disorganized, pivot toward automation that now requires a period of stabilization and rigorous evaluation. Clinical leaders must take an active role in the design of these algorithms to ensure that the “human in the loop” principle remains a cornerstone of British medicine. This involves creating feedback loops where doctors can correct AI errors in real-time, thereby refining the technology’s accuracy for future users. By prioritizing transparency and establishing clear legal accountability for AI-generated medical advice, the healthcare system can mitigate the risks associated with self-diagnosis. Ultimately, the successful integration of artificial intelligence will depend on its ability to enhance the physician’s reach without eroding the trust and safety that define the medical profession. Professionals should advocate for policies that ensure digital tools complement the clinical experience, ensuring that every patient, regardless of their tech-savviness, receives evidence-based and compassionate care.