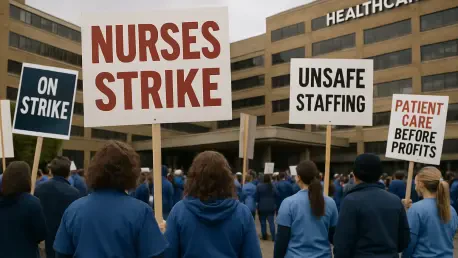

The conclusion of the largest nursing walkout in New York City history signaled a dramatic transformation in how metropolitan medical systems approach the fundamental rights and safety of frontline providers. For forty-one grueling days, the rhythmic chanting of thousands of New York State Nurses Association members echoed through the concrete canyons surrounding major facilities like Montefiore and Mount Sinai. This was not merely a dispute over hourly compensation; it was a localized manifestation of a national exhaustion that has been simmering within the nursing profession for years. By the time the final group of holdout workers at the New York-Presbyterian system ratified their deal with a ninety-three percent majority, the landscape of urban healthcare delivery had been permanently altered. The resolution of this conflict, involving nearly fifteen thousand professionals, serves as a masterclass in how collective bargaining can force a reckoning with the systemic vulnerabilities of modern medicine. Beyond the immediate return to work, the agreement established a blueprint for how large-scale private hospital systems must reconcile their operational budgets with the essential human cost of care. This movement was characterized by a rare unity that bridged the gap between different hospital networks, proving that the challenges of the profession were universal rather than institutional.
A New Standard for Economic and Physical Security
The financial core of the newly minted agreement addressed the immediate economic pressures facing the nursing workforce by securing a twelve percent salary increase over the three-year duration of the contract. However, the true victory for the union resided in the codification of enforceable safe staffing standards, which moved beyond simple recommendations to become legally binding obligations for hospital administrators. For years, the gap between patient volume and available staff had compromised the quality of bedside care, leading to the burnout that precipitated this historic strike. By institutionalizing these ratios, the contract provided a mechanism to penalize facilities that failed to maintain adequate personnel levels, thereby shifting the financial incentive toward retention rather than temporary patchwork solutions. This structural change ensured that the workload remained manageable, allowing nurses to provide the attentive care that complex medical cases require. The ripple effect of these staffing mandates is expected to influence labor negotiations across the northeastern seaboard, as other regional healthcare systems now face pressure to match these heightened standards or risk losing their top talent to the competitive New York City market.
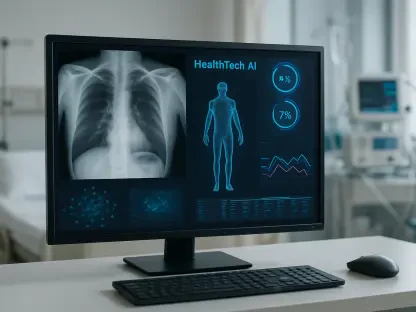
Beyond traditional labor concerns, this agreement introduced pioneering safeguards regarding the implementation of artificial intelligence and automated systems within the clinical environment. As hospitals increasingly look toward algorithmic tools for patient monitoring and predictive diagnostics, the New York State Nurses Association successfully negotiated for provisions that prevent technology from replacing professional clinical judgment or being used as a justification for reducing human staffing. These protections were critical in ensuring that emerging technologies serve as a support mechanism rather than a primary driver of care delivery, maintaining the human element that is indispensable in medical treatment. Furthermore, the contract significantly enhanced protections against workplace violence, an issue that has seen a disturbing rise in urban emergency departments. By mandating the installation of advanced security systems and establishing clear protocols for reporting and responding to incidents, the hospitals acknowledged that physical safety is a non-negotiable prerequisite for effective work. These measures represent a modern evolution of labor contracts, addressing the digital and physical realities of the contemporary workplace while setting a precedent for future technological integration.
Strategic Integration of Human and Technical Resources
The resolution of the dispute also forced a fundamental shift in the relationship between hospital management and the labor force, moving toward a model of mutual respect and enforced compliance. While hospital executives initially resisted the union’s demands, citing fiscal constraints and the need for operational flexibility, the persistent nature of the strike eventually highlighted the indispensable role that nurses play in the financial viability of these institutions. Governor Kathy Hochul and other state officials played a crucial role in emphasizing that public health stability is intrinsically linked to the well-being of the nursing workforce, particularly in a dense metropolitan area like New York. The focus has now transitioned from the heated rhetoric of the picket lines to the technicalities of contract enforcement, with oversight committees being established to monitor adherence to the new rules. This transition period is vital for rebuilding trust between the administration and the frontline staff, ensuring that the friction of the strike does not linger and impede the delivery of patient services. The long-term success of this agreement will depend on the transparency of these committees and the willingness of management to view nurses as strategic partners in healthcare reform.
Stakeholders eventually recognized that the path forward required a proactive investment in the nursing pipeline and the stabilization of hospital infrastructure through transparent resource allocation. This necessitated the implementation of rigorous data-tracking systems to ensure that the newly won staffing ratios were met in real-time, preventing the slow erosion of standards that often followed previous labor agreements. Hospitals moved to integrate advanced scheduling software that prioritized nurse well-being alongside patient needs, reflecting a broader shift toward sustainable operational practices. Future considerations for the industry involved the expansion of these labor protections to include support staff and other allied health professionals, recognizing that the entire ecosystem must be fortified to prevent future disruptions. Administrators learned that the costs of a prolonged strike far outweighed the investment required to maintain a satisfied and safe workforce. By prioritizing long-term retention strategies over short-term financial gains, medical institutions began to cultivate a more resilient environment capable of withstanding the pressures of an evolving healthcare landscape. These systemic improvements ensured that the hard-won victories of the strike translated into lasting benefits for patients and providers alike.